Solutions to the population health management challenge
25 March 2022
For the latest webinar in GGI’s New NHS ICS Series, we invited two leaders at the forefront of population health management, one of whom invented the Tesco Clubcard, to share their thoughts on the challenges and opportunities facing integrated care systems.
This week’s webinar in GGI’s New NHS ICS Series marked a turning point in the discussion about population health management. It was time, we felt, to stop describing the problem and start focusing on solutions.
Introducing the session, GGI CEO Andrew Corbett-Nolan said: “Many webinars about population health management tend to describe how deep the water is or isn’t it shocking and shouldn’t we do something about it. Too often when we talk about population health, we focus on the challenge not on solutions and opportunities.”
In 2018, GGI published a report in collaboration with IBM Watson, How population health management will deliver a sustainable NHS, in which we examined the six main interventions (set out below) for population health management and their transformative potential.
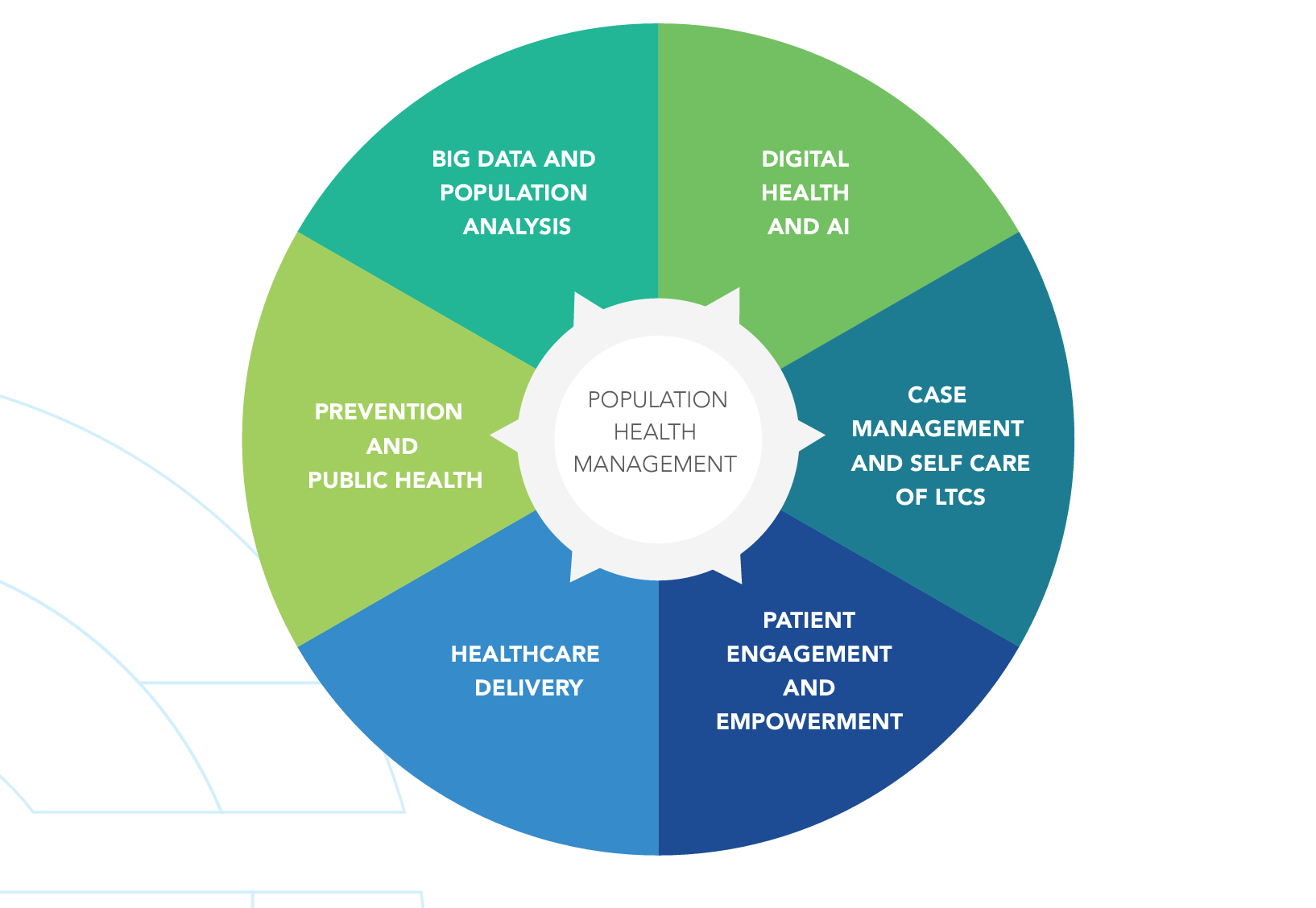
Integrated care systems in England are uniquely positioned to realise this potential and deliver on their key aims around improving population health and reducing health inequalities. But while ICSs will be the catalysts for this work, it will be powered and delivered on by providers – trusts, local authorities, VCSE organisations – working collaboratively and sharing intelligence.
Resetting population health
Our first speaker, Grant Harrison, co-founder of Reset Health, played a pivotal role in the development of the Tesco Clubcard – the original supermarket loyalty scheme. He is now using the experience to transform the health outcomes of people with type 2 diabetes and obesity in his work at Reset Health, an organisation driven by healthcare innovation to empower people to transform their own health.
Grant described the four areas he wanted to cover: “First, people are really complex, but you can get them to change en masse if you are clear about the behaviour you want and the benefits to them of making that change.
“Secondly, collecting and using data is awesomely interesting and awesomely challenging.
“Thirdly, you need new teams and processes and systems to achieve new stuff.”
Influencing behaviour – lessons from Tesco
Grant said: “In 1993 I was tasked with rethinking customer loyalty at Tesco and how we could persuade people to spend more money with us. The output of that was Tesco Clubcard, which launched in February 1995 and fundamentally changed supermarkets, and the behaviour of five million people.
“The two behaviours we wanted were very clear. One: shop more often; two: spend more on each trip. We got both of those behaviours. And most people said that they had not changed their behaviour at all. Why did they believe that? Because we focused on encouraging more of the behaviours that people were already doing.”
Data is king
“We focused on the household as the unit of measure, not the individual. Our decision-maker was very often the woman of the household. We knew through shopping analysis how often they would come in, their typical spending habits and, for example, whether they were a bargain hunter or an enthusiastic buyer of the latest products.
“I reckon that thinking about the household rather than the individual is also smart in healthcare – especially when healthcare is broadened to include what you eat, how you sleep, how you exercise and how you socialise.
“We quickly realised we had to reorganise to manage Clubcard, once we had moved from a 12-store trial to a national launch. We brought together the two customer insight departments: data analysis and market research. The behaviour data told us what people did, and the research data told us why they did it.
Learning by doing
“An interesting challenge for us in growing Clubcard was that there was no precedent. No one had done what we were doing and there was no academic research. We solved this problem by testing and learning as we went. We came up with ideas for what new services or products we should put in front of people and then we measured two things: how often do they come in and how much do they spend?
“We were also improving people’s trust in us. At one stage we were more trusted than the Bank of England. When we started Clubcard we were concerned about what people would think of us analysing their personal shopping data. What we found was very simple: as long as we kept the data safe - which we always did - we needed to show people that we were using their data to make shopping better for them. They understood the contract between us: I will give you data but show me how it benefits me and my family.
“Let’s talk about healthcare data. It’s way more than pills and medical procedures, as you know. It’s how much I move and play in my daily life, what and when I eat and drink, how I engage with friends and family, how I sleep and how I deal with stress.
“With Clubcard we analysed product 40,000 data points. I reckon that true healthcare will involve 10 times the breadth and depth of data – a truly massive amount. With machine learning and artificial intelligence, we have the capability to find links and causations that we’d never see otherwise so in healthcare we have more data and a responsibility to do more with it to help people.”
Mobile – the only game in town
When it comes to communication with customers, Grant said ‘the mobile phone is the only game in town’. He added: “I think the mobile phones and making social media and apps available to everyone are the gateway to scalable and impactful healthcare. They give us a chance to reach people when it will do the most good.
“Health happens every minute of every day and our phones are always there. They record and store health behaviours. They give us a chance to offer a word of support or ask a question at just the right time for each individual. Apps give clinical teams the opportunity to connect with patients when it really matters.
“You will remember that the two behaviours we wanted at Clubcard were to shop more often and spend more. What are the healthcare behaviours we want people to exhibit today in the UK? Here are three behaviours I think we need to see to keep people healthier and happier:
“One - keep curious: keep health top of mind, keep curious about your health and how it’s changing. You’re not a car whose servicing is outsourced to a mechanic.
“Two - keep on doing the healthy stuff. Do more of the healthy things you already do - taking your medicine, moving, eating good stuff, socialising with friends. You’re already doing great stuff, you just need to remember what it is and do more of it.
“Three - demand more from your clinical support system, whatever that is in your area and depending on your circumstances. I hope that as health move into everyday life, people will help us all continually improve to get better outcomes.”
Learning lessons from each other and elsewhere
Our second speaker, Bevleigh Evans, Head of Population Health Management at NHS England and NHS Improvement, agreed that understanding data is key – but added that it didn’t have to be complicated from the outset. She said: “We are working with the NHS and local authorities thinking about how you segment your population over their lifetime. In the Humber Coast and Vale they have divided their population into children and young people, adults working age and then older people and end of life. It can be that simple to start with.
“If we think about supporting families, we’re aware that if you think about obesity a child doesn’t have much control over what’s put on their plate. But if you take a family approach, like they did in Leeds pre-pandemic, and stat really working with families about creating shopping lists, thinking more broadly about cooking...
“What I found fascinating about the Leeds example is that they didn’t use obesity or ‘let’s lose some weight’ approach to this. They went into it with an outcome and worked backwards, working with families to establish how you could do a nudge effect to encourage healthier eating. So if you have three takeaways a week, let’s look at how we can work with you to bring it down to one per week.”
“Population health management isn’t an end in itself; no one wakes up thinking ‘I’ve got to do some great population health management today’. We get up because we care about our communities and want to make a difference to their outcomes. We need to think about how to move to equity rather than equality in how we address population health inequalities.
“I’ve been talking to systems about how they can do population health management through new ways of working. I spoke to Buckinghamshire, Oxfordshire and Berkshire West ICS yesterday and we spoke about how to bring together population health management, health inequalities and personalisation and prevention and how can the sum of the parts all support each other? They aren’t different things they are just a way of working that encompasses the whole patient group.”
Bevleigh also offered some valuable international perspective for those feeling bogged down by the challenge of integration. She said: “Six years ago, when I started this job, I was constantly reaching out globally to learn. In the last 18 months that’s really changed – I'm now being approached from all over the world so they can learn from us. And that’s thanks to all the hard work done by systems. Thinking about the shielding list, which was controversial at the time, but the Canadian Government said ‘it’s amazing you’ve been able to reach out and shield people because they’re at higher risk’. When I reflect about how worried we are about waiting lists, the Australians reflect back that at least you know what you know, we have so many private providers we don’t even know the scale of our issue.”
The next event in our New NHS ICS Series will take place on 30 March with a focus on place and provider collaboratives.